
From COVID-19 to HIV-1, Duke Surgical Sciences Blazes the Trail in Vaccine Immunology
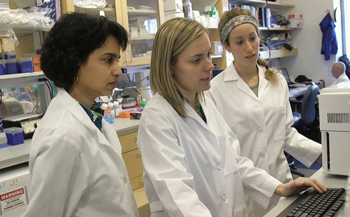
Photo above: The Center for Human Systems Immunology aims to understand the immune responses to infection and vaccination. Photo taken March 2020.
The COVID-19 vaccines are one of the greatest discoveries of the past 100 years. Their success has set new standards for how future vaccines should be designed and manufactured: a well-documented safety record, an excellent efficacy rate (up to 95%), and an accelerated production timeline compared with traditional vaccines. The novel mRNA technology that brought about this success was based on decades of research, including seminal work in the Division of Surgical Sciences.
Messenger RNA, or mRNA, is a single-stranded molecule of ribonucleic acid (RNA) present in all living things. In the COVID-19 vaccines, mRNA delivers the sequence of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike protein to the cell, which uses this harmless piece of code to construct the viral protein. The immune system then recognizes the processed viral protein on the cell as an unwelcome invader and mounts a robust response with immunological memory of the virus. The duration of the immune response elicited by the vaccine depends on how long this immune memory lasts.
A Gamechanger
Smita Nair, PhD, Professor in Surgery, Division of Surgical Sciences, first investigated the use of mRNA as a therapeutic in a cancer vaccine in 1995. The team in the Duke Department of Surgery included Dr. Nair, Dr. Eli Gilboa, and David Boczkowski. They were the first to create a cancer vaccine by transfecting dendritic cells with mRNA from the patient’s tumor and then injecting the cells back into the patient.

Professor in Surgery, Division of Surgical Sciences
“Labs were not testing RNA as vaccines at that time,” says Dr. Nair. “There were a couple of early papers, but not the way we were doing it; these studies involved direct injection of RNA into the body. However, there were no follow-up studies. We were putting mRNA in cells, which then produces the protein and processes it for immune recognition. Using mRNA and scaling up mRNA is easier and cheaper than protein.”
Their study showed proof of concept that dendritic cells could be used as an effective platform for administering RNA to patients with cancer. The first study was published in the Journal of Experimental Medicine in 1996 (Boczkowski et al., 1996). This research was later licensed to Argos Therapeutics, Inc. In contrast to a cell-based vaccine, the current COVID-19 vaccines deliver RNA by direct injection. However, their study was the first to show that RNA could be used as a vaccine and scaled up for mass production for clinical use.
"We showed that the dendritic cell–RNA vaccine works, and we can get an immune response that controls tumor growth. We also showed that this is an easy and very scalable strategy for any vaccine because if you know the sequence of the protein, you can easily make RNA in the lab in large quantities. We have done this for our cancer vaccine clinical trials. The RNA is made in the lab from a plasmid template using a standard process. The RNA is then stored in the freezer until use. This was discussed widely when the COVID-19 mRNA vaccines were being distributed."
- Smita Nair, PhD, Professor in Surgery
In addition to enabling the rapid and mass production of vaccines, RNA vaccines are safe because the RNA does not enter the cell’s nucleus. The cell makes protein from the RNA, which is then broken into pieces for immune recognition. Dr. Nair and her team have demonstrated the safety of the dendritic cell–RNA vaccine approach in their cancer vaccine trials since 1995.
Dr. Nair says the RNA field really took off at the turn of the century, which she deems the “RNAissance Period.”
“People were transitioning from using cells transfected with RNA to using direct injection of RNA,” explains Dr. Nair. “The explosion in the RNA field at the time was remarkable and continues to this day.”
RNA vaccines show promise as a breakthrough technology with other applications. Dr. Nair’s RNA vaccine approach has been used in brain, renal, and prostate cancer at Duke. The Duke RNA vaccine platform was confirmed and extended by several other labs. Worldwide, RNA vaccines are currently in clinical trials for infectious diseases, including HIV/AIDS, influenza, Zika, and rabies, and other cancers, including melanoma, breast, and lung (DeFrancesco, 2017).
A Lesson From Nature
Georgia Tomaras, PhD, Professor in Surgery, Division of Surgical Sciences, joined Duke in 1998 as a postdoctoral fellow in Dr. Michael Greenberg’s lab studying CD8 T cell immunity in patients with HIV-1 who were able to control virus replication all on their own without treatment.
Duke Surgery had a long history of innovative HIV/AIDS research, beginning with the discovery of AZT as the first treatment for HIV infection in 1985 in Dr. Kent Weinhold’s lab and the development of T20, or Fuzeon, as a first-in-class HIV-1 virus entry inhibitor in Dr. Dani Bolognesi’s and Dr. Tom Matthew’s labs.
“I joined the faculty in the Department of Surgery and the Division of Surgical Sciences since it was a place where multiple lab groups worked together to drive new discoveries and when possible translate them to clinical care,” says Dr. Tomaras. “I was able to start off immediately studying what naturally works well in the human immune response to infection as a guide to what a vaccine can do to reproduce that response in the whole population instead of just a few individuals.”
The Tomaras laboratory works with other research labs in the division and across Duke University to define protective antibody responses to HIV-1 vaccination. As part of the Duke Human Vaccine Institute, the lab made ground-breaking discoveries in the mechanisms of HIV-1 vaccine efficacy involving antibodies. They found that IgG3 antibodies correlated with a decreased HIV-1 acquisition risk, and specific IgA antibodies modulated the protective efficacy. These discoveries were transformative in revealing how a vaccine could educate the immune system to fight against infection.
In 2019, Dr. Tomaras co-founded the Center for Human Systems Immunology with Dr. Cliburn Chan in the Duke University School of Medicine. The center aims to map the immune experience during infection and vaccination to understand immunological resilience. The center provides expertise using cutting-edge immunological assays, integrated data management systems, and analytical approaches to understand protective immunity. “Specifically, we study how an intervention, such as a vaccine, will modulate the immune response and give an outcome of protection against disease,” says Dr. Tomaras.
As part of their center’s research portfolio, Dr. Tomaras oversees the immunology work of the largest ongoing HIV vaccine trials as part of the HIV Vaccine Trials Network (HVTN). There are multiple HIV-1 clinical efficacy trials looking to build upon the modest efficacy seen in a previous study in 2009.
“It's really been an unprecedented time I think for HIV research. In a relatively short period of time, the field has had two recently completed efficacy trials and two more ongoing. We now or will soon have in hand clinical outcome data that can help us understand the role of antibodies and interactions with Fc receptors in protection against disease.”
- Dr. Georgia Tomaras, Professor in Surgery
Dr. Tomaras and her team conduct immune correlates analyses to see if they can pinpoint a protection signal in the immune assays to better understand the efficacy of the HIV-1 vaccine regimen. By examining the antibody responses of the vaccine recipients, they can determine why certain recipients were protected at higher or lower levels. These results will aid in the design of future HIV-1 vaccine trials.
A New Threat
In a herculean effort, the scientists in Dr. Tomaras’ lab continued their HIV-1 vaccine research in addition to meeting the rapidly evolving situation with the emergence of COVID-19 over the past year. Her lab overcame operational challenges due to the pandemic to complete an immune correlates analysis for an HIV-1 efficacy trial that is helping to define the protective concentration of a passively infused monoclonal antibody.

The infrastructure and expertise they had built over decades for HIV-1 vaccine research was also readily available for COVID-19 vaccine research. Immunological tools were quickly adapted to be specific for COVID-19 and the quality assurance methods and data management strategies could be easily applied to studying the role of antibodies in protection against infection and severe disease.
"The effectiveness of the COVID-19 vaccines was so exciting and blew everybody out of the water," says Dr. Tomaras. "Considering the hurdles and low efficacy over the decades for HIV trials, the 95% efficacy for COVID-19 was astounding, and it's raised the bar for everything else. COVID-19 is very different from chronic HIV-1 disease and SARS-CoV-2 was seen as an easier virus target than HIV-1, but the level of efficacy and the efficiency of getting the clinical trial results was incredible. It raises the bar for how quickly our communities need to move from making and evaluating a vaccine. The inclusion of mRNA vaccines as part of this success will help the efforts for HIV-1 vaccine designs."
She says the HIV vaccine field is now increasing its efforts to use the same mRNA technology from the COVID-19 vaccine in a vaccine against HIV. The field has been using a number of approaches to elicit immune responses and while mRNA research is in the portfolio of potential approaches, it is now a top priority.
“People were doing that before COVID-19 so that's why COVID-19 research was able to move quickly,” says Dr. Tomaras. “mRNA had been tested with other pathogens, but it definitely has ramped up the conversation where everyone is more eager to try mRNA approaches.”
Give to Duke Surgery
A gift to the Department of Surgery is a gift of knowledge, discovery, and life.